
The status of the microbiocenosis of the female reproductive tract with threatened abortion in the first trimester of pregnancy: a descriptive, case-series study
20 February 2020
RESEARCH ARTICLE
The status of the microbiocenosis of the female reproductive tract with threatened abortion in the first trimester of pregnancy: a descriptive, case-series study
Iryna Romanenko1*, Oleg Golianovsky2
1Ukrainian Scientific and Practical Center for Endocrine Surgery, Transplantation of Endocrine Organs and Tissues of the Ministry of Health of Ukraine, Kiev, Ukraine;
2Department of Obstetrics and Gynecology no. 1, Shupyk National Medical Academy of Postgraduate Education, Kyiv, Ukraine.
Corresponding author:
Iryna Yurііvna Romanenko, PhD, associate professor
Leading researcher
Department of Reproductive Medicine and Surgery
Ukrainian Scientific and Practical Center for Endocrine Surgery, Transplantation of Endocrine Organs and Tissues of the Ministry of Health of Ukraine
13a, Klovskiy descent, Kiev, Ukraine, 02175
e-mail: iryna.roman2017@gmail.com
Short title: Microbiocenosis of reproductive tract in women with abortion imminence
What is not known, yet, about the topic
The causes of miscarriage in the first trimester of pregnancy cannot always be explained. A possible influence would be the condition of the vaginal microbiome, but this aspect is insufficiently studied.
Research hypothesis
The imminence of abortion in the first trimester of pregnancy could be associated with dysbiosis of the lower genital tract.
Article's added novelty on this scientific topic
The prevalence of microbiocenosis disorders in pregnant women with abortion imminent in the first trimester is 41.67%. Correcting dysbiosis could reduce the risk of miscarriage.
ABSTRACT
Introduction. The threatened abortion is the most common complication of pregnancy, which occurs in 15-20% of pregnancies and is associated with premature birth and low birth weight, pre-eclampsia, premature rupture of the membranes, placental abruption. According to researchers, microbiocenosis disorders in pregnant women lead to a complicated course of pregnancy, childbirth and the postpartum period, as well as the development of infectious and inflammatory processes in the mother and fetus. The purpose of this research was to study the state of the microbiocenosis of the genital tract in pregnant women with threatened abortions in the first trimester in order to improve therapeutic and preventive measures and to avoid obstetric and perinatal complications in such women.
Material and methods. The study included 24 pregnant women in the first trimester of pregnancy, who were hospitalized because of the threatened abortion in the hospitals, located in the Luhansk region. A comprehensive clinical and laboratory examination, assessment of the vaginal biocenosis by the bacterioscopic method and using the polymerase chain reaction with the help of the Femoflor-Screen test system in Real time mode were carried out.
Results. Five (20.83%) women complained about the presence of pathological discharge from the genital tract, 1 (4.17%) woman was concerned with itching and burning, 4 (16.67%) patients did not complain, but noticed that the amount of discharge from the genital tract increased slightly during the pregnancy. Clinical manifestations of vaginal microbiocenosis disorders (discharge, hyperemia) were observed in 8 (33.33%) patients. When using the microscopic method and the Femoflor-Screen test system, normocenosis was found in 14 (58.33%), nonspecific vaginitis – in 6 (25.00%), vaginal candidiasis – in 2 (8.33%), bacterial vaginosis – in 1 (4.17%) and trichomoniasis – in 1 (4.17%) woman. When comparing the results obtained using the microscopic method and the Femoflor-Screen test, concordant results were obtained for 20 (83.33%) samples, while in 4 (16.67%) cases – discordant results were obtained.
Conclusions. The prevalence of microbiocenosis disorders among pregnant women with threatened abortions in the first trimester was 41.67%. The combined use of the microscopic method and the Femoflor-Screen test system makes it possible, in most cases, to identify various forms of vulvovaginal and cervical infections with verification of the etiological factor, as well as to establish asymptomatic bacterial and candida carriage, which is crucial for the choice of treatment tactics.
Keywords: pregnancy, threatened abortion, vaginal microflora, microbiocenosis, laboratory diagnostics, polymerase chain reaction.
INTRODUCTION
The threatened abortion (TA) is the most common pregnancy complication, which occurs in 15-20% of the cases of ongoing pregnancy and is associated with premature birth, low birth weight, preeclampsia, premature rupture of the membranes and placental abruption [1]. Annually, 13 million children (10% of births) from the whole world are born prematurely [2]. Preterm birth is responsible for nearly half of all infant mortality in the United States [3].
Despite accomplishments in the study of etiology, pathogenesis, and the development of various methods of diagnosis and treatment of the threatened abortion, the frequency of miscarriage remains stable [4].
During pregnancy, estrogen and progesterone levels change, leading to physiological changes in the lower genital tract of pregnant women, such as a change in the pH, change in local immunity, which can sometimes lead to an increase in the concentration of anaerobic bacteria and other pathogenic microorganisms in the vagina [5, 6 , 7].
The Human Microbiome Project, completed in 2012, characterized the microbiome composition of various parts of the body of healthy people of different nationalities, including the vaginal microbiomes during the pregnancy [8]. It was established that the susceptibility to the adverse effects of pregnancy depends on the composition and structure of the vaginal microbiome during pregnancy. According to recent data, infection and changes in the immune system of the mucous membranes of the genital tract are considered as some of the main primary triggers of most preterm births [9, 10, 11].
A number of scientific publications have shown that dysbiotic changes in the vaginal microflora lead to a complicated course of pregnancy, childbirth and postpartum period, as well as to the development of infectious and inflammatory processes in the mother and fetus [12-15].
According to many authors, elucidating the relationship of the vaginal microbiocenosis with local and innate immunity, molecular and biological aspects, and the state of vaginal microcenosis will allow to predict the development of pathological processes, timely identifying pregnant women with a high risk of infectious and inflammatory complications, while early correction of vaginal dysbiosis will reduce the frequency of complications in the mother, fetus, and the newborn later on [16, 17, 18].
The purpose of the study was to examine the state of the microbiocenosis of the genital tract in pregnant women with threatened miscarriage in the first trimester in order to improve the therapeutic and prophylactic measures and to prevent the obstetric and perinatal complications in such women.
MATERIAL AND METHODS
We examined 24 women in the first trimester of pregnancy, who were hospitalized for threatened abortion in hospitals in the city of Rubezhnoye, Lisichansk, Luhansk region (Ukraine) in 2015-2016. Before the start of the examination, each subject signed an Informed Consent of the patient for conducting diagnostics, treatment and processing of personal data.
The criteria for inclusion in the main group were the woman’s informed consent, the presence of symptoms of threatened abortion and the gestational age, corresponding to the first trimester of pregnancy.
Observation and clinical examination of the women was carried out in accordance with the recommendations set forth in the Orders of the Ministry of Health of Ukraine on July 15, 2011 no. 417 “On the organization of ambulatory obstetric and gynecological care in Ukraine” and on November 3, 2008 no. 624 Clinical protocol “Miscarriage”. All pregnant women underwent a comprehensive clinical and laboratory examination – medical history, obstetric examination, clinical and biochemical blood tests, blood clotting tests, general urine test, bacterioscopic examination, vaginal and cervical canal examination by means of the real-time polymerase chain reaction using the “Femoflor Screen” test system.
The state of the vaginal microbiocenosis was evaluated according to the following criteria: total microbial contamination, dominant morphotypes, the presence of yeast cells, pseudomycelia filaments, epithelial and “key” cells, leukocytes. Disruption of the vaginal microbiocenosis was recorded if: (1) the prevalence of other microorganisms than lactobacilli was discovered and “key cells” were detected (bacterial vaginosis); (2) yeast cells and/or pseudomycelia of yeast-like fungi were detected while leukocytes prevailed over epithelial cells (vulvovaginal candidiasis); (3) the predominance of leukocytes over epithelial cells was observed (nonspecific vaginitis) [19].
A quantitative assessment of the vaginal biocenosis using a real-time polymerase chain reaction (RT-PCR) via the “Femoflor Screen” method included an assessment of the total bacterial mass of Lactobacillus spp. and major groups of microorganisms. Conditionally pathogenic flora was recorded, including facultative and obligate anaerobes, fungi, and absolute pathogens (Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis and Herpes viruses). Subsequently, the results of the study of vaginal biocenosis obtained by RT-PCR were interpreted.
Conclusion “normocenosis” was exhibited with a share of lactobacilli of more than 90% of the total bacterial mass (TBM), conditionally pathogenic aerobic and anaerobic microorganisms representing less than 10% of the TBM. Cases where the content of lactobacilli was over 90% of the TBM, mycoplasmas and/or fungi of the genus Candida were in an amount not exceeding 10% of the TBM, were taken as “relative normocenosis”. For the cases of “moderate aerobic dysbiosis” or “moderate anaerobic dysbiosis”, a decrease in the proportion of lactobacilli between 20% and 90% of TBM and an increase in the share of aerobes or anaerobes were taken. When the lactobacillus fraction was found to be lower than 20% of TBM and a sharp increase in the proportion of anaerobes was noted, the samples were evaluated as “pronounced anaerobic dysbiosis”, while an increase in the proportion of aerobes was considered as “pronounced aerobic dysbiosis” [20].
Statistical data processing was performed using SPSS 17.0 and Microsoft Excel for Windows (2013). Data are presented as mean and interquartile range (Q1-Q3, IQR).
RESULTS
The average age of the women was 26.0 (23.0-30.0) years. The largest number of patients was observed at the age of 20-30 years (16 women – 66.67%), that is, among the active and working part of the population. Secondary education was completed by 8 (33.33%) women, secondary special education – 10 (41.67%) women and higher education – 6 (25.00%) women, respectively. The vast majority of women were in a registered marriage – 21 (87.50%), the median duration of which was 2.0 (1.0-5.0) years.
The body mass index was 21.8 (20.5-25.0) kg/m2. The average age of the menarche in the group was 13.0 (12.0-14.0) years. The duration of the menstrual cycle was 28.0 (27.0-29.5) days, the duration of the menstrual bleeding was 5.0 (4.0-5.0) days, 1 (4.17%) woman characterized the blood loss quantity as little, 16 (66.67%) – as moderate, 7 (29.17%) – as profuse and 9 (37.50%) women reported dysmenorrhea.
Diseases of the gastrointestinal tract were noted in 2 (8.33%) patients, diseases of the liver and biliary tract – 2 (8.33%) patients, diseases of the respiratory tract – 4 (16.67%) patients, diseases of the urinary tract – 3 (12.50%) patients, thyroid hyperplasia of the 1st-2nd degree with euthyroidism in 2 (8.33%) patients and hay fever in 3 (12.50%) patients.
The median age of onset of sexual activity was 16 (16-18) years; most women reported the onset of sexual activity before marriage – 21 (87.50%) people. For 11 (45.83%) women, it was the first pregnancy. A history of childbirth was present in 11 (45.83%) patients, induced abortions – in 9 (37.50%) patients, spontaneous abortions – in 2 (8.33%) patients and miscarriages – in 3 (12.50%) examined patients.
From the suffered gynecological diseases, the most common were the pseudo-erosion of the cervix (7 people – 29.17%), salpingoophoritis (3 – 12.50%); functional ovarian cysts (5 – 20.83%), secondary infertility (1 – 4.17%), menstrual irregularities (1 – 4.17%), nonspecific vaginitis (1 – 4.17%) and urogenital candidiasis (2 – 8.33%).
Five (20.83%) patients complained of pathological discharge from the genital tract, 1 (4.17%) woman reported itching and burning, while 4 (16.67%) patients did not complain, but noticed that the quantity of secretions from the genital tract increased slightly during the pregnancy.
Clinical manifestations of disturbances of the vaginal microbiocenosis (discharge, hyperemia) were observed in 8 (33.33%) patients. During the clinical obstetric-gynecological examination, vaginal discharge of a grayish-white color, uniform consistency and unpleasant odor was noted in 1 (4.17%) case, curdled discharge was noticed in 1 (4.17%) case, and moderate, yellowish, homogeneous discharge was found in 7 (33.33%) cases.
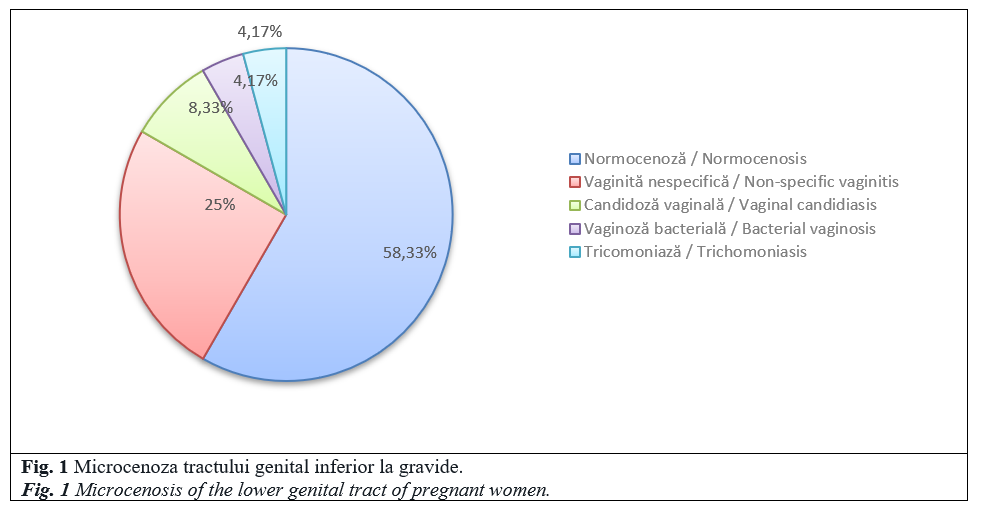
When using the microscopic method, normocenosis was detected in 14 (58.33%) pregnant women, nonspecific vaginitis – 6 (25.00%) pregnant women, vaginal candidiasis – 2 (8.33%) pregnant women, bacterial vaginosis – 1 (4.17%) pregnant woman and trichomoniasis – 1 (4.17%) pregnant woman (Figure 1).
In the microscopic examination of patients with normal vaginal microcenosis, lactoflora prevailed over other microorganisms, while all the markers of dysbiosis were absent. In the case of nonspecific vaginitis, smear microscopy indicated a local inflammatory reaction of varying severity (the number of leukocytes was in the range from 50 to half of the visual field). In the case of vaginal candidiasis, the presence of blastospores and filaments of mycelium was noted, while in bacterial vaginosis – mixed microflora, a low number of leukocytes, the presence of “clue cells“ and a low number of lactobacilli were detected. In one case, inconsistency of clinical and microscopic data was noted (the presence of an insignificant amount of blastospores and mycelial filaments without clinical manifestations), which suggests asymptomatic candida carriage.
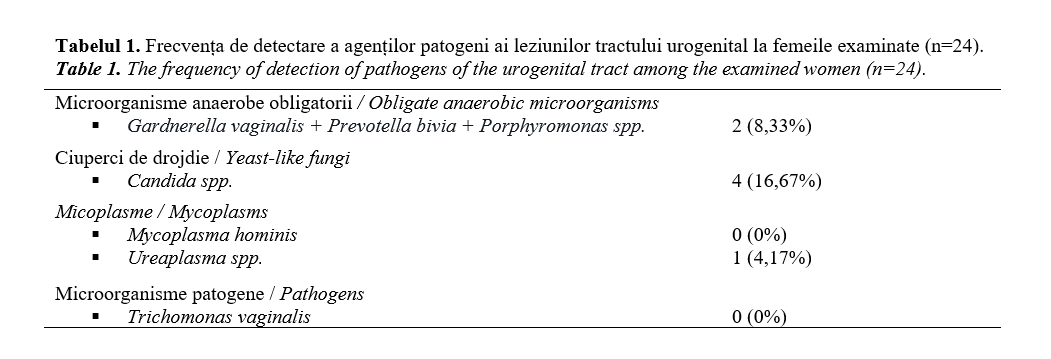
Analyzing the results of the study using the Femoflor-Screen test, it should be noted that the total bacterial mass in the studied samples was determined in the range from 107 to 108 decimal logarithms of the concentration, the number of lactobacilli varied from 104 to 108 lg, respectively, the proportion of lactobacilli was in the range from 40% to 90% of TBM. The Femoflor-Screen test revealed clinically significant amounts of representatives of opportunistic microflora. The frequency of detection of pathogens of lesions of the urogenital tract is presented in Table 1.
When comparing the results obtained using the microscopic method and the Femoflor-Screen test, concordant results were obtained for 20 (83.33%) samples, and in 4 (16.67%) cases, discordant results were obtained.
According to the results of direct microscopy, “key cells” were found in 1 sample, while the Femoflor-Screen test testified to the normal ratio of bacterial mass and lactobacilli. One sample gave the opposite result: when using the Femoflor-Screen test, the presence of Ureaplasma spp. was detected, while at the same time, using the microscopic method, physiological microbiocenosis was noted. In addition, it is worth noting that in 2 samples, the Femoflor-Screen test found an exceeded threshold of Candida spp., and neither the clinical picture nor the microscopic examination data confirmed the presence of urogenital candidiasis in women. Therefore, we can consider the asymptomatic bacterial and candida carriage.
DISCUSSION
Our studies of the microcenosis of the lower genital tract in pregnant women with TA confirmed the data of Pestrikova T. et al. [21] that the microbiota is not identical and is depending on the presence of nosological forms (nonspecific vaginitis, vaginal candidiasis, bacterial vaginosis, trichomoniasis), which is of fundamental importance for the choice of therapeutic strategies.
Using the microscopic method and the Femoflor-Screen test system, normocenosis was detected in 14 (58.33%) pregnant women, nonspecific vaginitis was present in 6 (25.00%) women, vaginal candidiasis was present in 2 (8.33%) women, bacterial vaginosis was present in 1 (4.17%) woman and trichomoniasis was found in 1 (4.17%) woman. Our results regarding the prevalence of bacterial vaginosis in the first trimester were consistent with data from Donders G. et al. – 8.4% [22], however, they differ from the results of Karapetyan T. et al. [23], who found normocenosis in 36.4%, bacterial vaginosis – in 40.3%, vaginal candidiasis – in 12.9%, and nonspecific vaginitis – in 10.4% of pregnant women in the first trimester. Our data confirm the opinion of Nenadić D. et al. [24] on the need for an integrated approach to the identification of patients with inflammation of the lower genital tract.
The results of our study showed the need to assess vaginal biocenosis at the beginning of the pregnancy, regardless of clinical symptoms and classifying women with a dysbiotic state as a risk group for adverse pregnancy and childbirth outcomes. This approach will allow to take corrective measures by influencing the identified changed indicators, and will contribute to improving the antenatal monitoring system for women with threatened abortion.
CONCLUSIONS
The prevalence of microbiocenosis disruptions among pregnant women with TA in the first trimester is 41.67%. Using the microscopic method and the Femoflor-Screen test system, normocenosis was found in 58.33% of the pregnant women, nonspecific vaginitis – in 25.00%, vaginal candidiasis – in 8.33%, bacterial vaginosis – in 4.17%, trichomoniasis – in 4.17% of women. Asymptomatic bacterial and candida carriage was found in 16.67% of cases.
The use of complex clinical and laboratory examination methods allows, in most cases, to identify various forms of vulvovaginal and cervical infections with verification of the etiological factor, as well as to establish asymptomatic bacterial and candida carriage, which is of fundamental importance for the choice of the therapeutic strategy.
An antenatal study of the microflora of the reproductive system and surveillance of infectious and non-infectious lesions of the lower reproductive tract will allow to individualize the approach to management and to develop, if necessary, corrective measures that will contribute to the successful completion of pregnancy, positively influencing the health of the mother and her offspring.
Declaration of conflicting interests
Nothing to declare.
Authors` contribution
Both authors participated equally in the study and in the drafting of the manuscript. The final version of the article was read and approved by both authors.
References
- Ahmed S., El-Sammani M., Al-Sheeha M., Aitallah A., Jabin Khan F., Ahmed S. Pregnancy outcome in women with threatened miscarriage: a year study. Mater. Sociomed., 2012; 24 (1): 26-8. doi:10.5455/msm.2012.24.26-28.
- Goldenberg R., Hauth J., Andrews W. Intrauterine infection and preterm delivery. New Engl. J. Med., 2000; 342: 1500-1507.
- Behrman R., Butler A. Institute of Medicine (US) Committee on understanding premature birth and assuring healthy outcomes. Washington (DC): National Academies Press (US); 2007. Preterm birth: causes, consequences, and prevention.
- Mathews T., MacDorman M. Infant mortality statistics from the 2005 period linked birth/infant death data set. Natl. Vital. Stat. Rep., 2008; 57: 1-32.
- Anderson B., Mendez-Figueroa H., Dahlke J., Raker C., Hillier S., Cu-Uvin S. Pregnancy-induced changes in immune protection of the genital tract: defining normal. Am. J. Obstet. Gynecol., 2013; 208 (4): 321-329. doi:10.1016/j.ajog.2013.01.014.
- Galiñanes S., Coppolillo E., Cifarelli M., Cora Eliseht M., Pellisa E., Losada M. et al. Vaginal inflammatory status in pregnant women with normal and pathogenic microbiota in lower genital tract. ISRN Obstet. Gynecol., 2011; 835-92 doi:10.5402/2011/835926.
- Wen A., Srinivasan U., Goldberg D., Owen J., Marrs C., Misra D. et al. Selected vaginal bacteria and risk of preterm birth: an ecological perspective. J. Infect. Dis., 2014; 209 (7): 1087-1094. doi:10.1093/infdis/jit632.
- Prince A., Chu D., Seferovic M., Antony K., Ma J., Aagaard K. The perinatal microbiome and pregnancy: moving beyond the vaginal microbiome. Cold Spring Harb. Perspect. Med., 2015; 5 (6): a023051. doi:10.1101/cshperspect.a023051.
- Macintyre D., Chandiramani M., Lee Y., Kindinger L., Smith A., Angelopoulos N., Lehne B., Arulkumaran S., Brown R., Teoh T., Holmes E., Nicoholson J., Marchesi J., Bennett P. The vaginal microbiome during pregnancy and the postpartum period in a European population. Sci. Rep., 2015; 5: 8988. doi:10.1038/srep08988.
- Wei S., Fraser W., Luo Z. Inflammatory cytokines and spontaneous preterm birth in asymptomatic women – a systematic review. Obstet. Gynecol., 2010; 116: 393-401.
- Xu F., Du X., Xie L. Vaginitis in pregnancy is related to adverse perinatal outcome. Pak. J. Med. Sci., 2015; 31 (3): 582-586. doi:10.12669/pjms.313.6752.
- Larsson P., Bergstrom M., Forsum U., Jacobsson B., Strand A., Wolner-Hanssen P. Bacterial vaginosis. Transmission, role in genital tract infection and pregnancy outcome: an enigma. APMIS, 2005, 113 (4): 233-245.
- Donders G. Definition and classification of abnormal vaginal flora. Best Pract. Res. Clin. Obstet. Gynaecol., 2007; 21: 355-73.
- Lamont R., Sobel J., Akins R., Hassan S., Chaiworapongsa T., Kusanovic J., Romero R. The vaginal microbiome: new information about genital tract flora using molecular based techniques. BJOG, 2011; 118 (5): 533-49. doi:10.1111/j.1471-0528.2010.02840.x.
- Svare J., Schmidt H., Hansen B., Lose G. Bacterial vaginosis in a cohort of Danish pregnant women: prevalence and relationship with preterm delivery, low birthweight and perinatal infections. BJOG, 2006; 113 (12): 1419-1425. doi:10.1111/j.1471-0528.2006.01087.x.
- Simhan H., Caritis S. Prevention of preterm delivery. N. Engl. J. Med., 2007; 357: 477-87.
- Thorsen P., Vogel I., Olsen J., Jeune B., Westergaard J., Jacobsson B. et al. Bacterial vaginosis in early pregnancy is associated with low birth weight and small for gestational age, but not with spontaneous preterm birth: a population-based study on Danish women. J. Matern. Fetal Med., 2006; 19: 1-7.
- Mijović G., Lukić G., Jokmanović N., Crnogorac S., Kuljić-Kapulica N., Gajić M. et al. Impact of vaginal and cervical colonization / infection on preterm delivery. Vojnosanit. Pregl., 2008; 65 (4): 273-280.
- Savicheva A., Vorobeva N., Vagoras A., Sokolovskiy E., Gallen A., Domeyka M. Ispol`zovanie metoda pryamoy mikroskopii urogenital`nyih mazkov na ambulatornom priyome s tsel`yu optimizatsii diagnostiki urogenital`nyih infektsiy [Using direct microscopy of urogenital smears at an outpatient clinic to optimize the diagnosis of urogenital infections]. Trudnyiy patsient [Difficult patient], 2008; 6 (1): 9-12 (in Russian).
- Boldyireva M., Donnikov A., Tumbinskaya L. Femoflor. Issledovanie biotsenoza urogenital`nogo trakta u zhenschin metodom PCR s detektsiey rezul`tatov v rezhime real`nogo vremeni. Metodicheskoe posobie dlya laborantov [The study of the biocenosis of the urogenital tract in women by the polymerase chain reaction with the detection of results in real time. Methodical manual for laboratory assistants]. M.; 2009, 77 p. (in Russian).
- Pestrikova T., Yurasova E., Kotelnikova A. Harakteristika mikrobioty i vlagalischa pri sochetanii bakterial`nogo vaginoza s patologiey vlagalischa i sheyki matki vospalitel`nogo geneza. [Characteristics of the vaginal microbiota with a combination of bacterial vaginosis with the pathology of the vagina and cervix inflammatory genesis]. Ginekologiya [Gynecology]. 2017; 19 (4): 15-19. DOI:10.26442/2079-5696_19.4.15-19. (in Russian).
- Donders G., Van Calsteren K., Bellen G., Reybrouck R., Van den Bosch T., Riphagen I., Van Lierde S. Predictive value for preterm birth of abnormal vaginal flora, bacterial vaginosis and aerobic vaginitis during the first trimester of pregnancy. BJOG, 2009; 116 (10): 1315-24. doi:10.1111/j.1471-0528.2009.02237.x.
- Karapetyan T., Ankirskaya A., Muravyova V. Bakterial`nyiy vaginoz v pervom trimestre beremennosti [Bacterial vaginosis in the first trimester of pregnancy]. Meditsinskiy sovet [Medical Council], 2015 (XX): 68-71. https://doi.org/10.21518/2079-701X-2015-XX-68-71. (in Russian).
- Nenadić D., Pavlović M. Cervical fluid cytokines in pregnant women: relation to vaginal wet mount findings and polymorphonuclear leukocyte counts. European Journal of Obstetrics Gynecology and Reproductive Biology, 2008; 140 (2): 165-170.