
Comparative analysis of the characteristics of rotaviral infection in vaccinated and non-vaccinated infants: prospective, descriptive study
20 February 2020
RESEARCH ARTICLE
Comparative analysis of the characteristics of rotaviral infection in vaccinated and non-vaccinated infants: prospective, descriptive study
Tatiana Alsaliem1,2*, Ala Donos1, Constantin Spînu4, Ninel Revenco1, Valentin Turea1, Ion Mihu1, Radu Cojocaru3, Stela Gheorghita3, Albina-Mihaela Iliev3
1Department of pediatrics, Nicolae Testemitanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova;
2Municipal Children's Clinical Hospital no. 1, Chisinau, Republic of Moldova;
3Nicolae Testemitanu State University of Medicine and Pharmacy, Chisinau, Republic of Moldova;
4National Agency for Public Health, Chisinau, Republic of Moldova.
Corresponding author:
Tatiana Alsaliem, paediatrician
Acute diarrheal diseases unit
Municipal Children's Clinical Hospital no. 1
7, Serghei Lazo str., Chisinau, Republic of Moldova, MD-2004
e-mail: banaritania@yahoo.com
Short title: Comparative analysis of the characteristics of rotaviral infection in infants
What is not known yet, about the topic
The genetic variability of rotaviral infection in infants up to and after vaccination is unknown, as well as the evolution of this virus depending on genotype, phenotype, and patient’s immune status, presence of comorbidities in infants, up to and after vaccination.
Research hypothesis
Vaccination of population by rotaviral vaccine modify clinical and paraclinical rotaviral infection characteristics, as well as the pathogen genotype.
Article’s added novelty on this scientific topic
The article presents data on the influence of vaccination on rotaviral genotype and phenotype in the Republic of Moldova, as well as aspects of the clinical-paraclinical evolution of rotaviral infection in pre- and post-vaccinated infants.
ABSTRACT
Introduction. Acute diarrheal disease is one of the most current health problems of the baby. Rotaviral infection is the most common cause of dehydration in infants and young children. The implementation of the sentinel surveillance of rotaviral infection in infants from 2008 in the Republic of Moldova demonstrated the high rate of this infection (40.0%), being an argument in recommending the antirotaviral immunization in children within the National Immunization Program.
Material and methods. The study enrolled children with acute diarrheal disease, included in the sentinel supervision (2012-2016) and treated in the Unit of acute diarrheal diseases of Clinical Children's Hospital no. 1. Were assessed 193 patients with acute diarrheal disease, according with a standard clinical approach. The biological material was examined by serological enzyme-linked immunosorbent assay (ELISA) and genotyping revealed by polymerase chain reaction (PCR).
Results. The rotaviral infection was confirmed in 193 infants, of which 121 children were not vaccinated against rotaviral infection, and 72 were immunized. Depending on the genotypes encountered before and after vaccination, it was found that G9P[8], G3P[8], G4P[8] was detected before vaccination, but post-vaccine prevailed G2P[4], G4P[8], also the incidence of rotaviral infection is decreasing, and the evolution of the disease is much easier.
Conclusions. This article reflects the evolution of the genotypic properties of rotaviruses and the clinical-paraclinical particularities of rotaviral infection in infants, with a major importance in the context of the implementation of antirotaviral immunization in children within the National Immunization Program in the country.
Key words: diarrhea, rotavirus, children, infants, vaccine.
INTRODUCTION
The health of society and future generations is largely dependent on the health of new-borns and children, which is closely correlated with a multitude of factors [1]. The evaluation of the illnesses among the children of the first year of life marks an increased incidence of the bronchopulmonary pathology, being followed by the infections of the gastrointestinal tract [2]. The involvement in the epidemiological process of the young children, attests a major economic and epidemiological importance of the rotaviral infection. According to WHO data, around 10027 cases of deaths in children up to 5 years old are caused by the rotaviral infection in Europe. In the countries of the European Union (EU), in children up to 5 years old, there are 2.8 million rotaviral infections, resulting in more than 200 deaths, 87,000 hospitalizations.
The problem of rotaviral infection remains current during the last 45 years, since the discovery of this virus has been associated with an increased incidence, especially among children up to 5 years old [3]. Each child can withstand from one to several episodes of the disease, characterized by a high incidence of serious cases, with complications and lack of specific antirotaviral therapy. In the rotaviral infection extra-intestinal disorders occur, involving not only the mucosa of the gastrointestinal tract, but also the respiratory, cardiac, reno-urinary system, nervous system, liver, pancreas, spleen [4].
Vaccines are the only public health prevention strategy that can control rotaviral disease. They have been developed to imitate immunity as a result of natural rotavirus infection, which provides protection against severe gastroenteritis and therefore reduces the risk of primary care, hospitalization, and death [5].
MATERIAL AND METHODS
Prospective, descriptive study, included 193 children with acute diarrheal disease, involved in the sentinel surveillance (2012-2016) from the Acute diarrheal diseases unit, Clinical Municipal Children's Hospital no. 1.
The research protocol was approved by the Research Ethics Committee of the Nicolae Testemitanu SUMPh from the Republic of Moldova (report no. 54 of 13.02.2017, president of REC – Viorel Nacu, PhD, assoc. prof.).
All patients were selected according to the standard case scenario. The hospitalization rules and the completion of a standardized questionnaire for this study were respected. The parents of the children gave written informed consent for their enrollment in the research.
The criteria for inclusion in the study were:
- age from 1 month to 12 months (the age of the baby was established according to WHO recommendations) [6];
- diarrhea with at least 3 defecations in the last 24 hours, but not more than 7 days;
- patients examined by serological reaction ELISA with genotypes detected in PCR for rotaviral infection within the first 24 hours after admission;
The criteria for exclusion of patients from the research:
- patients with rotaviral infection or severe comorbidities (heart defects, digestive tract development abnormalities, nervous system development abnormalities, etc.).
- patients with diarrhea of less than 3 fluid defecations in the last 24 hours.
The presence of signs of dehydration was appreciated in the children included in the study, at the time of the clinical examination,. The evaluation of the degree of dehydration in acute diarrheal disease according to the WHO is as follows: severe – lethargic, has closed eyes, cannot drink or drink with difficulty, the skin fold returns to normal very slowly (>2 sec); moderate – agitated or irritable, has eyes closed, drinks with greed, thirst, skin fold returns to normal slowly (<2 sec) [7].
The biological material of all the children included in the study was virologically examined for rotaviral infection, using the ELISA serological reaction and genotyping in the chain polymerization reaction (ProSpecT ROTAVIRUS Kit, manufacturer – Zhejiang Orient Gene Biotech Co., LTD, China). This is a qualitative immunoenzymatic test for the detection of rotavirus (group A) in human faecal samples as an aid in the diagnosis of acute gastroenteritis. The assay uses a polyclonal antibody to detect group-specific proteins, including the main internal capsid protein (VP6), present in group A rotaviruses [8].
About 1.5-2 ml of liquid faeces or 1 g of fresh semi-formed faeces, spontaneously emitted were collected in a sterile recipient from each patient, on the first day of hospitalization. The container was hermetically sealed, labelled with patient data and stored at 2-8˚C until transport. Also, for each patient with positive results for rotaviral infection, the status of the vaccine was established by questioning the caregiver with whom the child was admitted to the hospital, checking the child's development booklet and checking the vaccination register at the residence place.
Depending on the vaccine status, the study sample (n=193) was divided into group “Unvaccinated children with rotaviral infection” (n=121) and group “Vaccinated children with rotaviral infection” (n=72).
Sample size was estimated, using the formula:
n=[1/(1-ƒ)×2(Zα+Zβ)2×P(1-P)/(P0-P1)2]
n=[1/(1-0,1)×2(1,96+0,84)2×0,625×0,375/(0,50-0,75)2]=65
where:
Po – according to the bibliographic data [9], the success of the treatment in the unvaccinated patients constitutes on average 50.0% (P0=0.50);
P1 – expected success of treatment in the vaccinated children group will be 75.0% (P1=0.75); P=(P0+P1)/2=0.625;
Zα – table value. When the statistical significance is 95.0%, then the coefficient Zα=1.96;
Zβ– table value. When the statistical power of the comparison is 80.0%, then the coefficient Zβ=0.84.
ƒ – Proportion of subjects expected to abandon the study for reasons other than the investigated effect q=1/(1-ƒ), ƒ=10.0% (0.1).
Therefore, the L1 research group will include no less than 65 patients vaccinated against rotaviral infection and the L0 control group will include no less than 65 unvaccinated patients.
The data collected in the study were entered into the electronic table through the Microsoft Office Excel 2007 program. The results were processed using the SPSS version 22 software. For comparing the differences between groups, the 95% confidence interval (95CI), the criterion (csi-square) χ2 was calculated. The significance threshold was considered p<0.05.
RESULTS
In both groups, male sex prevailed. Depending on age, in the unvaccinated group, children aged 6-12 months predominated in 66.9% cases, compared to the vaccinated group, where this age group constituted only 47.2%.
The patients included in the study were admitted to the hospital during the first 3 days of illness. In all patients, the disease started with acute intoxication syndrome in 100% of the cases in unvaccinated children compared with 82% in the vaccinated children, characterized by alteration of the general condition, decreased appetite and general weakness.
Table 1 shows the much more severe evolution of the unvaccinated children who supported the rotaviral infection, compared with the vaccinated ones, thus the moderate and severe dehydration constituting 53.7% vs. 30.6% in the vaccinated group. The clinical form in which rotaviral infection occurred was manifested by gastro-enterocolitis in 81% of unvaccinated and 75% of those vaccinated.
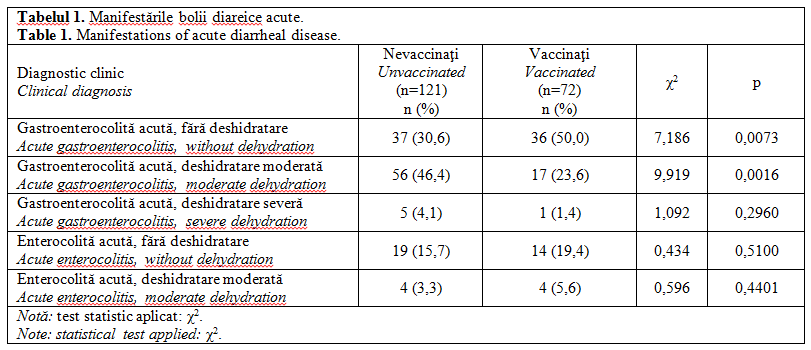
The distribution of patients depending on the basic clinical diagnosis is shown in Table 1.
In unvaccinated children vomiting was present in 80%, fever – in 76.9%, faeces with pathological inclusions – in 97.5%, whereas in vaccinated children these symptoms were less frequent (Table 2).
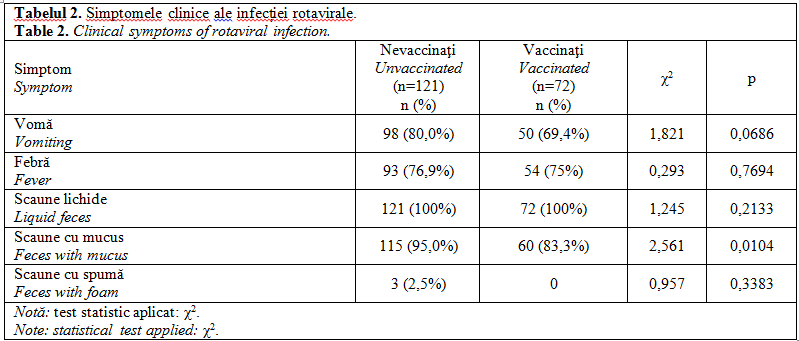
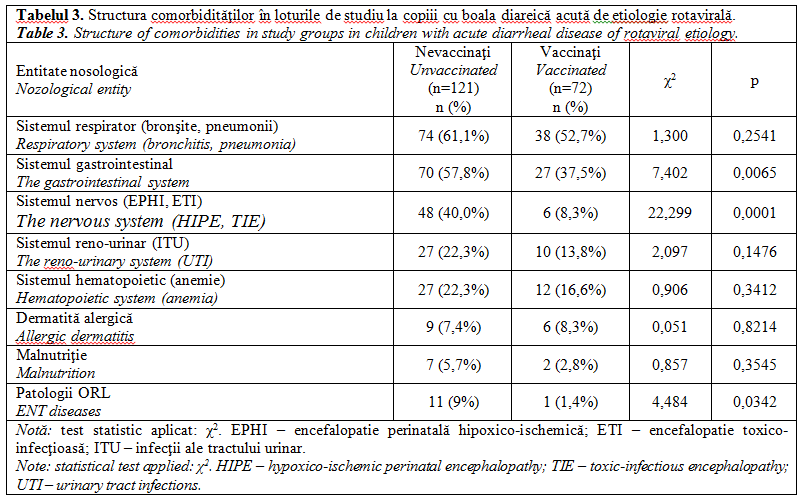
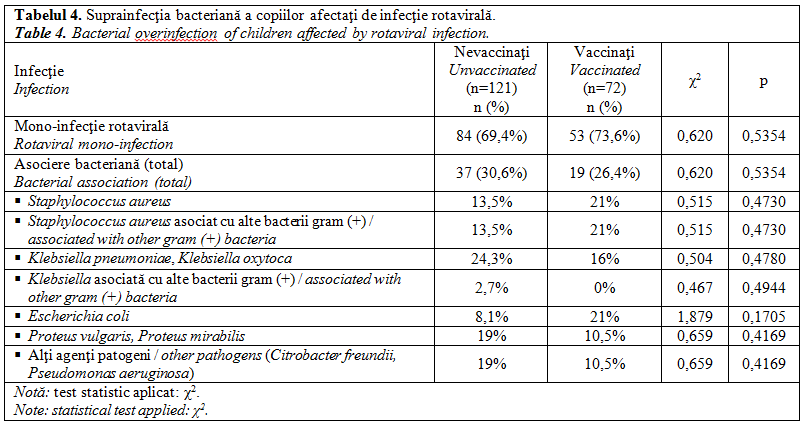
Table 3 shows the frequency of comorbidities that occurred concurrently with rotaviral infection. There is a predominance of pathologies of the respiratory system (bronchitis, pneumonia) with an incidence of 61.1%, followed by pathologies of the gastrointestinal system with 57.8%, the third place being the pathologies of the nervous system (perinatal hypoxic-ischemic encephalopathy, toxic-infectious encephalopathy).
Most unvaccinated children were in the hospital for a double period of time compared to those vaccinated. Thus, the average length of hospitalization in the group of unvaccinated children was 6.7 days, while in the vaccinated children the average duration was 6 days.
The rotaviral etiology of acute diarrheal disease was confirmed in all patients included in the study. In 73.6% of cases of acute diarrheal disease of viral etiology, bacterial flora was associated, more significantly in unvaccinated children. Thus, in the unvaccinated group, Klebsiella pneumoniae and Proteus mirabilis predominated with 5%, double compared with the vaccinated
group, followed by Staphylococcus aureus and Citrobacter freundii at a rate of 4%. In 2.5% atypical h+ Escherіchіa colі and Klebsiella oxytoca were detected. The etiological structure of rotaviral infection is shown in Table 4.
In the performed study, acetonuria was found in 47 unvaccinated children vs. 20 vaccinated children. Thus, ketone bodies in the urine in marked quantity (≥150 mg/dl) were found in 21.3% of the cases in the unvaccinated group, compared with 5% in the children from the vaccinated group.
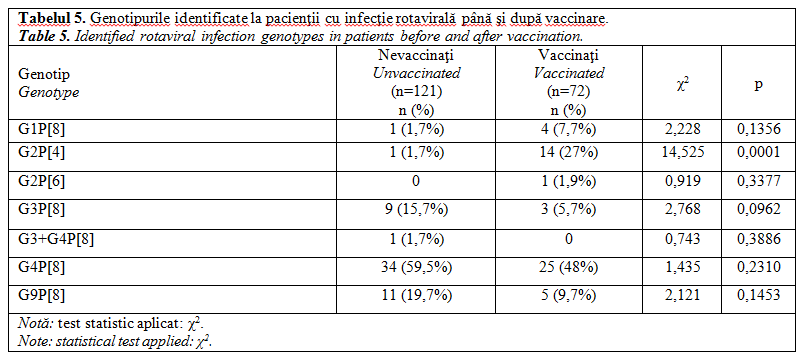
Of the total number of genotypes samples, the incidence of genotypes identified in patients with rotaviral infection during the prevaccinal period, the most commonly encountered genotypes were G4P[8], G3P[8] and G9P[8]. In the post-vaccine period, their frequency decreased in the first place, being the genotypes G2P[4] and G4P[8]. The incidence of genotypes identified in patients with rotaviral infection up to and after vaccination is shown in Table 5.
 DISCUSSION
DISCUSSION
Rotavirus is one of the most important causative agents of acute dehydrating diarrheal disease and is involved in 12.0-71.0% of acute hospitalized gastroenteritis cases. In developed countries rotaviruses cause from 1/3 to 1/2 of all serious diarrhea. Thus, about 3 million cases of rotaviral infection (RVI) are registered annually in the USA, which causes 67 thousand hospitalizations (250 thousand day/bed) and more than 100 cases of deaths [10].
In 2006, two live attenuated vaccines were developed and authorized: Rotarix® and RotaTeq®. Rotarix is a monovalent vaccine derived from a human G1P isolate [8]. RotaTeq® is a pentavalent, consisting of a mixture of mono-reassortants human bovine rotavirus, which transports genes encoding human G1, G2, G3, G4 and P[8] proteins into a genetic background of Wi79 bovine rotavirus (G6P[5]). Both vaccines have proven to be very effective in clinical trials and have been included in the mandatory national vaccination scheme for children in over 100 countries since 2006. Post-marketing studies have shown that both vaccines are highly effective at the population level.
Moldova was the first country in the WHO European Region to introduce rotavirus vaccination into the routine immunization program for children. In the vaccine used in Moldova are present the genotypes G4, G2, G9 that cover most strains of circulating rotaviruses in the population of the country according to the monitoring and sentinel surveillance data in children up to the age of 5 years.
According to our data, this is the first research study of patients with rotaviral infection even after vaccination in the Republic of Moldova and who analyzed the prophylactic potential of the antirotaviral vaccine in our country. Given that vaccines have been very effective in high-income
countries, they have proven to be considerably less powerful in low- and middle-income countries. The disease associated with rotavirus was the cause of death in> 200,000 children aged <5 years worldwide in 2013.
According to a study realised by Ulrich Desselberger, it was established that while vaccine effectiveness was high in high-income countries, with severe rotavirus disease protection rates at 80-90%, in low- and middle-income countries it was by 30-50% lower. Different factors were analyzed here that were identified or suggested to be involved in the differences in efficacy of the rotaviral vaccine, including malnutrition, intestinal microbiota status, vitamin D3 administration, co-infections, immunity of the infant immune system and genetic factor [11].
Raúl F. Velázquez performed a systematic review and meta-analysis to describe, compare and synthesize the effectiveness of the vaccine, from randomized clinical trials prior to authorization, finding a decrease in hospitalizations and addresses to the children's emergency department. with rotaviral infection [12].
Another study carried out in the neighboring country Romania (2014) by Victoria Birlutiu and Rares Mircea Birlutiu between January 1, 2011 – December 31, 2012, aimed at tracking the seasonality of the disease, the clinical aspects, the severity of the disease, the laboratory examinations, the need for parenteral rebalancing, the costs of hospitalization. The study group consisted of 236 children (2011 – 114 cases, 2012 – 122 cases) between 0 and 16 years old with rotaviral infection in the infectious diseases services in children in Sibiu. Thus, 114 cases were diagnosed in 2011, respectively 122 in 2012, more frequently in the cold months, more frequently in the male gender, sex ratio M/F 1.42:1 in 2011, 1.18:1 in 2012, in the group aged 1-3 years – 58.90%. 91 cases in 2011 – 79.82%, respectively 112 cases in 2012 – 91.80% with an average / severe score. Fifteen cases showed neurological manifestations, 15 cases acute renal failure. Severe onset cases led to hospitalization in the first 24 hours: 41.23% of cases in 2011 and 51.64% in 2012, prolonged with diarrhea over 6 days-it was established in 62 cases (54.39%) in 2011 and 75 cases (61.48%) in 2012. Cases with severe dehydration were found in children aged 1 to 12 months, being associated with thrombocytopenia, leukopenia, PCR increase (probability 0.42), hydro-electrolyte imbalances associated with signs of encephalopathy. This study highlights the frequent association of hyponatremia (<130 mEq/l) from electrolyte imbalance with rotavirus gastroenteritis, 83 cases in 2011 and 51 cases in 2012. In this context it is worth mentioning that in Romania the rotaviral vaccine was not included in National Immunization Program [13].
The study peformed by Stela Gheorghita obtained results that indicate a favorable impact of the vaccination program on rotaviral disease in children from Chisinau, Moldova. Two-dose rotavirus vaccination reduced hospitalization by 79%, and severe disease progression was reduced by 82%. Overall, hospitalizations with rotavirus decreased by two-thirds until the second year of the program, in a model compatible with the impact of the vaccine. The decrease was the largest of the vaccinated cohort's children <1 year in the first year and <2 years in the second year after vaccine implementation. In addition, there were clear decreases in the number of rotavirus hospitalizations for all children <5 years old, including unvaccinated cohorts, suggesting indirect protection resulting from immunization of children [1].
Estimation of the efficacy of 2-dose vaccination in Moldova, especially against severe cases at 84% (95% CI: 65% to 93%), is largely compatible with the estimates of vaccine effectiveness in other countries with low mortality (in the mortality layers A and B of WHO) VE is 85% (95% CI: 80% to 88%) based on the overall analysis of 8 studies, including >32,000 participants [14].
CONCLUSIONS
The morbidity due to the rotaviral infection (RVI) decreased considerably as a result of the implementation of the rotaviral vaccine, keeping the seasonality of the infection in the cold period of the year with the increased affect in the infant after 6 months.
Clinical progression of rotaviral infection was easier in vaccinated vs. unvaccinated infants. As a result of the vaccination according to the National Immunization Program, the rotaviral strains circulating in the country have changed. The results of the study reconfirmed the need to implement the Rotarix vaccine containing G4, G2, G9 genotypes through the National Immunization Program (y. 2012) in order to reduce the burden of rotaviral infection on the health system in the Republic of Moldova.
Declaration of conflicting interests
Nothing to declare
Authors' contribution
Study design (AD, NR, IM, VT), accumulation of clinical materials (AD, TA, CS, SG), data interpretation and statistical analysis (AD, TA), preparation of the manuscript (SG, AMI, RC). The final version of the manuscript was read and approved by all authors.
REFERENCES
- Gheorghiţa S., Bîrca L., Donos A. et al. Impact of rotavirus vaccine introduction and vaccine effectiveness in the Republic of Moldova. Clinical Infectious Diseases, 2016; 62 (suppl. 2): S140.
- Denisyuk N. Genetic characteristics of rotaviruses of group A circulating in the Orenburg region during the 2016-2017 season. Infections in Infants, 2017; 16 (4).
- WHO. Diarrhea (Newsletter). April 2017.
- Uciaikin V., Novokshonov A. Antiinflammatory therapy in complex therapies for the treatment of viral infections and viral-bacterial infections. Infections in Infants, 2012; Special Issue.
- Grimwood K., Lambert S., Milne R. Rotavirus infections and vaccines: burden of illness and potential impact of vaccination. Rotavirus Infections and Vaccines, 2010; 12 (4): 235-256.
- WHO. Early child development. 2013.
- WHO Vaccine-Preventable Diseases Surveillance Standards, September 5, 2018.
- Remel Diagnostic Tests, Thermo Scientific Oxoid Microbiology Products 2019.
- Dozornii epidnadzor za rotavirusnoi infectsiei v Respublike Moldova (iuni 2008 – avgust 2015) Natsionalinii Tsentr Obshestvenovo Zdorovia 6-oe soveshceanie Evropeiskovo reghionalinovo biuro VOZ po dozornomu epidnadzoru za rotavirusnoi infectsiei.
- Bîrca L., Spînu C., Rusu G. et al. Infecţia rotavirală – particularităţi clinico-epidemiologice şi opţiuni de profilaxie. Anale Ştiinţifice ale USMF ,,Nicolae Testemiţanu”, 2008; 3(9): 324-328.
- Desselberger U. Differences of rotavirus vaccine effectiveness by country: likely causes and contributing factors. Pathogens, 2017; 6 (4): 65.
- Velázquez R., Linhares A., Muñoz S., Seron P., Lorca P. Efficacy, safety and effectiveness of licensed rotavirus vaccines: a systematic review and meta-analysis for Latin America and the Caribbean. BMC Pediatrics, 2017; 17: 14.
- Bîrluţiu V., Bîrluţiu R. Underevaluated rotavirus infection in Romania: prospective clinical and epidemiological study, therapeutic and economic implications. Acta Medica Transilvanica, 2014; 19 (1): 154-156.
- Soares-Weiser K., Maclehose H., Bergman H. et al. Vaccines for preventing rotavirus diarrhoea: vaccines in use. Cochrane Database Syst Rev 2012; 11.